Biological Bases of Behavior: Nervous and Endocrine Systems (7A)
Help Questions
MCAT Psychological and Social Foundations › Biological Bases of Behavior: Nervous and Endocrine Systems (7A)
A patient presents with a rare autoimmune disorder that specifically targets and destroys Schwann cells. Which of the following physiological changes would most likely be observed in this patient's peripheral nervous system?
Increased speed of saltatory conduction.
Decreased resistance to ion leakage across the axonal membrane.
Enhanced neurotransmitter reuptake in the synaptic cleft.
Rapid regeneration of damaged motor neurons.
Explanation
A is correct. || What type of problem is this? This is a knowledge application question testing your understanding of myelination in the peripheral nervous system. The key is knowing what Schwann cells do and reasoning backward from their loss. || How to get the right answer: Schwann cells produce myelin in the PNS. Myelin wraps around axons and functions as an electrical insulator — it dramatically increases resistance to ion leakage across the axonal membrane, which is what makes saltatory conduction between Nodes of Ranvier possible. Destroy the Schwann cells, destroy the myelin, and ions that should stay put now leak freely through the bare axonal membrane. The result is a dramatic decrease in resistance to ion leakage — Choice A. || The traps: Choice B (increased speed of saltatory conduction) is the exact opposite — saltatory conduction depends on myelin to function. Without Schwann cells, conduction slows or fails entirely. Choice C (enhanced neurotransmitter reuptake) is unrelated to myelination — reuptake occurs at the synapse, not along the axon. Choice D (rapid regeneration) is a plausible-sounding distractor because PNS neurons can regenerate, but regeneration is slow and depends on surviving Schwann cells to guide it — if Schwann cells are destroyed, regeneration would be impaired, not rapid. || Strategy Rx: For Schwann cell questions, always anchor to the two core functions: (1) myelination (electrical insulation, enabling saltatory conduction) and (2) regeneration guidance. If the question destroys Schwann cells, both functions are lost — expect slower conduction and impaired regeneration, never enhanced speed.
Which of the following neurotransmitters is primarily responsible for the inhibitory tone of the central nervous system, and which ion channel does it typically open to achieve this?
Glutamate; voltage-gated Na+ channels.
Acetylcholine; voltage-gated Ca2+ channels.
GABA; ligand-gated Cl- channels.
Dopamine; ligand-gated K+ channels.
Explanation
C is correct. || What type of problem is this? This is a two-part recall question testing neurotransmitter identity and ion channel mechanism. Both parts must be correct — if either half of the paired answer is wrong, the whole choice is eliminated. || How to get the right answer: GABA (gamma-aminobutyric acid) is the primary inhibitory neurotransmitter in the CNS. When GABA binds its ionotropic receptor (GABA-A), it opens ligand-gated Cl- channels. Cl- is more concentrated outside the cell, so it flows inward when channels open. This influx of negative charge hyperpolarizes the membrane — makes the inside more negative — moving the potential away from the action potential threshold and inhibiting firing. Both halves of Choice C are correct. || The traps: Choice A names glutamate, the primary excitatory neurotransmitter — the opposite of what the question asks. Choice B names dopamine, which is a modulatory monoamine, not a primary inhibitory transmitter, and its mechanism does not primarily involve K+ channels in the way described. Choice D names acetylcholine, which at the neuromuscular junction opens Na+ channels (excitatory), and does not open voltage-gated Ca2+ channels as the primary mechanism of inhibition. || Strategy Rx: On paired neurotransmitter/ion channel questions, eliminate immediately if either half is wrong — don't try to decide if "most" of the answer is correct. Here: identify the inhibitory NT (GABA), then identify its ion (Cl- influx → hyperpolarization). Any choice with an excitatory NT or an excitatory ion channel mechanism is automatically wrong.
During a high-stress fight-or-flight scenario, the adrenal medulla is stimulated to release catecholamines. Which division of the nervous system is responsible for this stimulation, and what is the primary embryonic origin of the adrenal medulla?
Enteric; Mesoderm.
Sympathetic; Ectoderm (Neural Crest).
Parasympathetic; Mesoderm.
Somatic; Endoderm.
Explanation
B is correct. || What type of problem is this? This is a two-part embryology and autonomic nervous system question. Both the neural pathway and the developmental origin must be correct. This is a high-yield fact combination that appears frequently on the MCAT. || How to get the right answer: The adrenal medulla releases catecholamines (epinephrine and norepinephrine) as part of the fight-or-flight response, which is mediated by the sympathetic division of the ANS. The sympathetic system directly innervates the adrenal medulla via preganglionic fibers — the chromaffin cells of the medulla are essentially modified postganglionic sympathetic neurons. The embryonic origin is the key MCAT fact: the adrenal medulla derives from neural crest cells, which are an ectodermal (specifically neuroectodermal) derivative. The adrenal cortex, by contrast, is mesodermal. || The traps: Choice A (parasympathetic) is wrong because the parasympathetic system mediates rest-and-digest, not fight-or-flight. Choice C (somatic) is wrong because the somatic NS controls voluntary skeletal muscle, not glandular secretion. The mesoderm/endoderm options in Choices A, C, and D are all wrong because neural crest cells — the correct origin — arise from ectoderm. The most common error is confusing the mesodermal adrenal cortex with the ectodermal adrenal medulla. || Strategy Rx: Memorize this pairing as a unit: adrenal cortex = mesoderm = steroids (cortisol, aldosterone); adrenal medulla = neural crest (ectoderm) = catecholamines (epi, norepi). The medulla is essentially a sympathetic ganglion that secretes into the blood instead of onto a target organ.
A researcher uses a drug that acts as a potent selective serotonin reuptake inhibitor (SSRI). What is the immediate effect of this drug on the synapse?
Increased duration of serotonin signaling at the postsynaptic receptor.
Increased degradation of serotonin by monoamine oxidase (MAO).
Decreased concentration of serotonin in the synaptic cleft.
Competitive inhibition of the postsynaptic serotonin receptors.
Explanation
C is correct. || What type of problem is this? This is a pharmacology mechanism question testing your understanding of what reuptake inhibition does at the synapse. The key is tracing the consequence of blocking removal of the neurotransmitter from the cleft. || How to get the right answer: The reuptake transporter normally removes serotonin from the synaptic cleft back into the presynaptic neuron, terminating its signal. An SSRI blocks this transporter. When the transporter is blocked, serotonin cannot be removed from the cleft — it stays there longer and continues binding to postsynaptic receptors. The immediate result is an increased duration of serotonin signaling. More serotonin remains active at the receptor for a longer period of time. || The traps: Choice A (increased MAO degradation) describes the mechanism of MAO inhibitors (MAOIs), a different drug class. SSRIs and MAOIs both increase synaptic serotonin but through entirely different mechanisms. Choice B (decreased synaptic serotonin) is the opposite of what an SSRI does — blocking reuptake increases, not decreases, cleft concentration. Choice D (competitive inhibition of postsynaptic receptors) describes a receptor antagonist, which would block serotonin signaling — the opposite effect. SSRIs work at the presynaptic transporter, not at the postsynaptic receptor. || Strategy Rx: On reuptake inhibitor questions, always reason in two steps: (1) the transporter removes NT from cleft; (2) blocking the transporter = NT stays in cleft longer. The result is always increased concentration and increased duration of action. Any answer describing decreased signaling or degradation is automatically wrong for a reuptake inhibitor.
Following a traumatic brain injury, a patient is able to produce speech that is fluent and follows grammatical rules, but the speech is nonsensical and the patient has difficulty understanding spoken language. Which brain region was likely damaged?
The basal ganglia in the midbrain.
Broca's area in the frontal lobe.
Wernicke's area in the temporal lobe.
The occipital lobe's primary visual cortex.
Explanation
B is correct. || What type of problem is this? This is a clinical neuroscience question testing your ability to match a symptom profile to the correct brain region. The two-part clinical picture — fluent but nonsensical speech plus impaired comprehension — is the diagnostic signature of a specific aphasia type. || How to get the right answer: The patient produces speech that is fluent and grammatically intact but semantically nonsensical (word salad), and cannot understand spoken language. This is Wernicke's aphasia (receptive aphasia), caused by damage to Wernicke's area in the posterior superior temporal lobe. Wernicke's area is responsible for language comprehension — when damaged, the patient cannot decode incoming language or monitor whether their own speech makes sense. || The traps: Choice A (Broca's area) is the most common wrong answer because Broca's is the other major language area. But Broca's aphasia produces the opposite profile: speech is halting, effortful, and non-fluent (telegraphic), but comprehension is relatively preserved. The fluency of the speech is the critical differentiator — fluent word salad = Wernicke's; halting non-fluent speech = Broca's. Choice C (basal ganglia) affects motor coordination and procedural memory, not language. Choice D (occipital lobe) processes vision, not language. || Strategy Rx: Memorize the Broca's/Wernicke's contrast as a single paired fact: Broca's = production problem (can't speak well, can understand); Wernicke's = comprehension problem (can speak fluently but nonsensically, can't understand). The word "receptive" in Wernicke's aphasia refers to receiving/understanding language.
Which structure in the limbic system acts as the relay station for all sensory information, with the exception of olfaction?
Amygdala
Thalamus
Hippocampus
Hypothalamus
Explanation
A is correct. || What type of problem is this? This is a neuroanatomy recall question testing a high-yield fact about the thalamus's role as sensory relay station. The exception (olfaction) is the critical detail that makes this question tricky. || How to get the right answer: The thalamus is the sensory relay center of the brain — it receives signals from all major sensory modalities (vision via the lateral geniculate nucleus, hearing via the medial geniculate nucleus, somatosensation via the ventral posterior nuclei, taste) and routes them to the appropriate cortical areas for conscious processing. The critical exception is olfaction: smell is the only sense that bypasses the thalamus and projects directly to the olfactory cortex and limbic structures (amygdala, hippocampus). This explains why smell is so powerfully and directly linked to memory and emotion. || The traps: Choice B (hippocampus) is involved in memory consolidation and spatial navigation, not sensory relay. Choice C (amygdala) processes emotional significance of stimuli and is involved in fear conditioning, not general sensory relay. Choice D (hypothalamus) regulates homeostasis, hunger, thirst, temperature, and hormone release via the pituitary — not sensory relay. || Strategy Rx: The thalamus fact has two required components: (1) it relays all sensory information to cortex, and (2) olfaction is the sole exception. The olfaction exception is tested frequently precisely because it's counterintuitive and easy to overlook. Commit both parts to memory as a paired fact.
Chronic deficiency in dietary iodine leads to a goiter and reduced metabolic rate. This occurs because the biological basis of metabolism is heavily regulated by hormones produced in the:
Adrenal cortex.
Pancreas (Islets of Langerhans).
Thyroid gland.
Posterior pituitary.
Explanation
C is correct. || What type of problem is this? This is a hormonal physiology question testing your knowledge of which gland regulates basal metabolic rate and the role of iodine in hormone synthesis. || How to get the right answer: The thyroid gland produces thyroid hormones T3 (triiodothyronine) and T4 (thyroxine), which are the primary regulators of basal metabolic rate in virtually every cell of the body. Iodine is a structural component of these hormones — T3 contains 3 iodine atoms, T4 contains 4. Without adequate dietary iodine, the thyroid cannot synthesize these hormones, metabolic rate drops, and the gland enlarges (goiter) as TSH continues to drive stimulation of a gland that cannot respond. || The traps: Choice A (posterior pituitary) releases ADH and oxytocin — neither regulates metabolic rate. Choice B (adrenal cortex) produces cortisol and aldosterone, which affect stress response, glucose mobilization, and fluid balance — not basal metabolic rate. Choice D (pancreatic islets) produce insulin and glucagon, which regulate blood glucose acutely — not basal metabolic rate. A common error is selecting the adrenal cortex because cortisol affects glucose metabolism, but cortisol is a stress hormone that mobilizes glucose, not a regulator of the overall metabolic rate. || Strategy Rx: Metabolic rate = thyroid. This is a one-to-one pairing. Any question about slow metabolism, fatigue, cold intolerance, or goiter should immediately activate: thyroid → T3/T4 → iodine requirement.
Based on Experiment 1, what is the independent variable?
The presence or absence of gut microbiota.
The expression of BDNF in the hippocampus.
The activity level of the Vagus nerve.
Anxiety-like behavior in the plus-maze.
Explanation
B is correct. || What type of problem is this? This is a research design question testing your ability to identify the independent variable — the factor the researcher deliberately manipulates. You will recognize it by questions asking about experimental design components (IV, DV, control group, confound). || How to get the right answer: The independent variable is what the researcher controls and changes to observe its effect. In Experiment 1, the researchers created two groups: germ-free (GF) mice raised without any gut bacteria, and specific pathogen free (SPF) mice with normal gut microbiota. The only thing the researchers deliberately manipulated was the microbial status of the mice. Everything else (housing conditions, maze, measurement method) was held constant. The presence or absence of gut microbiota is the IV. || The traps: Choice A (anxiety-like behavior in the plus-maze) is the dependent variable — the outcome being measured, not the factor being manipulated. Choice C (BDNF expression) is a dependent variable from Experiment 2, not from Experiment 1 at all — it was not measured in this experiment. Choice D (Vagus nerve activity) was neither manipulated nor measured in Experiment 1. || Strategy Rx: On IV/DV questions, always use the manipulation test: ask "What did the researcher change or control?" That's the IV. Then ask "What did the researcher measure to see if the change had an effect?" That's the DV. Never confuse outcomes (DVs) with manipulations (IVs).
The Vagus nerve is a primary component of which nervous system division?
Central nervous system.
Sympathetic nervous system.
Somatic nervous system.
Parasympathetic nervous system.
Explanation
C is correct. || What type of problem is this? This is a neuroanatomy recall question testing your knowledge of cranial nerve classification. The Vagus nerve's division assignment is a high-yield MCAT fact. || How to get the right answer: The Vagus nerve (Cranial Nerve X) is the longest cranial nerve and is the workhorse of the parasympathetic division of the autonomic nervous system. It innervates the heart (slowing rate), lungs, and most of the abdominal viscera. It carries both efferent signals (brain to organs, slowing heart rate, promoting digestion) and afferent signals (organs to brain, including from the gut — the basis of the gut-brain axis described in this passage). The word "vagus" comes from Latin for "wandering," reflecting how widely it travels through the body. || The traps: Choice A (somatic nervous system) controls voluntary skeletal muscle — the Vagus does not innervate skeletal muscle (except for a small contribution to pharyngeal and laryngeal muscles). Choice B (sympathetic system) is the fight-or-flight system — the Vagus is the opposite, mediating rest-and-digest. Choice D (central nervous system) refers to the brain and spinal cord — the Vagus is a peripheral nerve. || Strategy Rx: Cranial nerve X (Vagus) = parasympathetic = rest and digest. This is one of the most frequently tested cranial nerve facts on the MCAT. Also memorize: the Vagus is the primary afferent pathway for the gut-brain axis — it carries signals from the gut upward to the brain, not just downward.
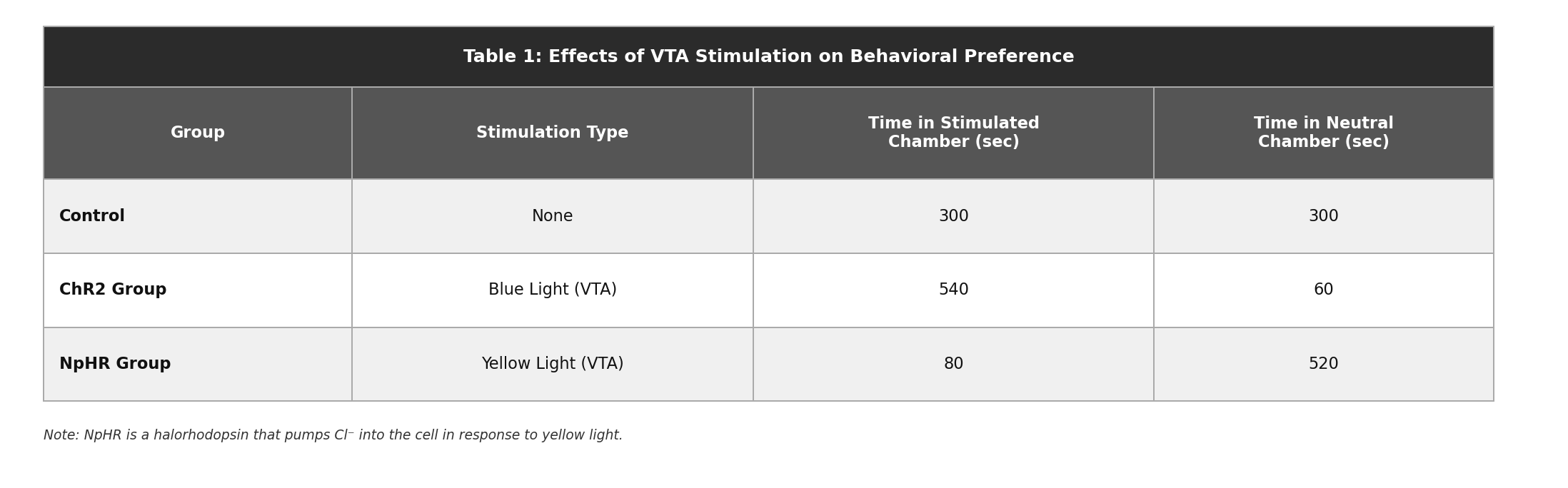
The pulse of blue light in the ChR2 group leads to which neuronal event in the VTA?
Depolarization and the firing of an action potential.
Inhibition of voltage-gated Ca2+ channels.
Hyperpolarization of the membrane.
Synthesis of new dopamine receptors.
Explanation
B is correct. || What type of problem is this? This is an optogenetics physiology question that requires you to trace the consequence of opening a specific ion channel. The question tests basic membrane physiology — what happens when Na+ channels open — in a novel experimental context. || How to get the right answer: ChR2 (Channelrhodopsin-2) opens Na+ channels in response to blue light. Na+ is more concentrated outside the cell than inside (~145 mM extracellular vs. ~12 mM intracellular), so it flows inward when channels open. This influx of positive charge depolarizes the membrane — makes the inside more positive — moving it toward the action potential threshold. If depolarization reaches threshold, the neuron fires an action potential. In the VTA context, firing dopaminergic neurons release dopamine into the Nucleus Accumbens, producing the rewarding effect observed in Table 1. || The traps: Choice A (hyperpolarization) would require an influx of negative ions (Cl-) or efflux of positive ions (K+) — Na+ influx does the opposite, depolarizing rather than hyperpolarizing. This confusion is exactly what the NpHR halorhodopsin tests in Q17. Choice C (inhibition of Ca2+ channels) is a mechanism associated with some inhibitory pathways but is not what Na+ channel opening does. Choice D (synthesis of new receptors) is a long-term genomic response, not an immediate electrophysiological consequence of light stimulation. || Strategy Rx: Ion channel questions follow a simple decision tree: (1) which ion enters or exits? (2) is that ion positive or negative? (3) influx of positive or efflux of negative = depolarization; influx of negative or efflux of positive = hyperpolarization. Na+ influx = positive charge entering = depolarization = excitation.